
Demographic study of hemorrhoid with analysis of risk factors
Abstract
Background: Hemorrhoids are the most prevalent benign anorectal disorder diagnosed in clinical practice. Risk factors commonly associated with hemorrhoidal disease include low fiber diet, chronic constipation & diarrhea, straining during defecation, pregnancy, sedentary lifestyle, obesity etc. Treatment of symptomatic first-degree, second degree and early third-degree hemorrhoids includes banding and sclerotherapy. Patients with fourth-degree or large third-degree hemorrhoids should be referred for hemorrhoidectomy surgery.
Methods: This retrospective study was conducted in the department of surgery in J.K. Hospital Bhopal. 430 adult patients with diagnosis of hemorrhoids, admitted in surgery ward were included in this study. All the relevant details were obtained from medical record department with all demographic details.
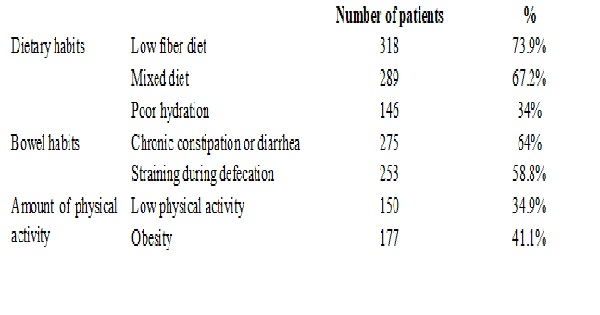
Results: Most of the patients (46%) belongs to the younger age (20-40 years). 69% were male patients and 31% were female patients. Patients with higher socioeconomic status were most commonly affected group (37.2%) with hemorrhoids. Commonest symptoms was Bleeding per rectum. In the present study, risk factors for hemorrhoids were low fiber diet, mixed diet, poor hydration, chronic constipation or diarrhea, straining during the defecation, low physical activity and obesity. Sclerotherapy (11.1%) and rubber band ligation (4.1%) were non operative treatment. Operative procedures performed in the present study were open hemorrhoidectomy (81.4%) and stapled hemorrhoidopexy (3.2%).
Conclusion: This demographic study of hemorrhoidal disease in this region can guide us to better understand the trends of this disease which is most commonly encountered in our society.This useful information may aid in the assessment and definitive care of these patients with hemorrhoids.
Downloads
References
2. Nikooiyan P, Sardo HM, Poursaeidi B, Zaherara M, Ahmadi B. Evaluating the safety, efficacy and complications of electrotherapy and its comparison with conventional method of hemorrhoidectomy. Gastroenterology and Hepatology from bed to bench. 2016;9(4):259-67.
3. Khan RM, Itrat M, Ansari AH, Zulkifle M, Ethisham. A study on associated risk factors of haemorrhoids. J Biol Sci Opinion. 2015;3(1):36-8.
4. Banov Jr L, Knoepp Jr LF, Erdman LH, Alia RT. Management of hemorrhoidal disease. Journal of the South Carolina Medical Association (1975). 1985 Jul;81(7):398.[pubmed]
5. Jacobs D. Clinical practice. Hemorrhoids. N Engl J Med. 2014 Sep 4;371(10):944-51. doi: 10.1056/NEJMcp1204188.[pubmed]
6. Rivadeneira DE, Steele SR, Ternent C, et al. Practice parameters for the management of hemorrhoids (revised 2010). Dis Colon Rectum. 2011 Sep;54(9):1059-64. doi: 10.1097/DCR.0b013e318225513d.[pubmed]
7. Altomare DF, Roveran A, Pecorella G, et al. The treatment of hemorrhoids: guidelines of the Italian Society of Colorectal Surgery. Tech Coloproctol. 2006 Oct;10(3):181-6. Epub 2006 Sep 20. DOI:10.1007/s10151-006-0277-y.
8. Buntzen S, Christensen P, Khalid A, et al. Diagnosis and treatment of haemorrhoids. Dan Med J. 2013 Dec;60(12):B4754.[pubmed]
9. Wald A, Bharucha AE, Cosman BC, ACG clinical guideline: management of benign anorectal disorders. Am J Gastroenterol. 2014 Aug;109(8):1141-57; (Quiz) 1058. doi: 10.1038/ajg.2014.190. Epub 2014 Jul 15.[pubmed]
10. Wald A, Bharucha AE, Cosman BC, et al. ACG clinical guideline: management of benign anorectal disorders. Am J Gastroenterol. 2014 Aug;109(8):1141-57; (Quiz) 1058. doi: 10.1038/ajg.2014.190. Epub 2014 Jul 15.[pubmed]
11. Ali SA, Shoeb MF. Study of risk factors and clinical features of hemorrhoids. International Surgery Journal. 2017 May 24;4(6):1936-9.
12. Johanson JF, Sonnenberg A. Constipation is not a risk factor for hemorrhoids: a case-control study of potential etiological agents. Am J Gastroenterol. 1994 Nov;89(11):1981-6.[pubmed]
13. Lohsiriwat V. Hemorrhoids: from basic pathophysiology to clinical management. World J Gastroenterol. 2012 May 7;18(17):2009-17. doi: 10.3748/wjg.v18.i17.2009.[pubmed]
14. Kann BR, Whitlow CB. Hemorrhoids: diagnosis and management. Techniques in Gastrointestinal Endoscopy. 2004 Jan 1;6(1):6-11.
15. Lestar B, Penninckx F, Kerremans R. The composition of anal basal pressure. An in vivo and in vitro study in man. Int J Colorectal Dis. 1989;4(2):118-22.[pubmed]
16. Loder PB, Kamm MA, Nicholls RJ, et al. Haemorrhoids: pathology, pathophysiology and aetiology. Br J Surg. 1994 Jul;81(7):946-54.[pubmed]
17. Loder PB, Kamm MA, Nicholls RJ, et al. Haemorrhoids: pathology, pathophysiology and aetiology. Br J Surg. 1994 Jul;81(7):946-54.[pubmed]
18. Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology. 1990 Feb;98(2):380-6.[pubmed]
19. Peery AF, Sandler RS, Galanko JA, et al. Risk Factors for Hemorrhoids on Screening Colonoscopy. PLoS One. 2015 Sep 25;10(9):e0139100. doi: 10.1371/journal.pone.0139100. eCollection 2015.[pubmed]
20. Riss S, Weiser FA, Schwameis K, et al. The prevalence of hemorrhoids in adults. Int J Colorectal Dis. 2012 Feb;27(2):215-20. doi: 10.1007/s00384-011-1316-3. Epub 2011 Sep 20.[pubmed]
21. Kaidar-Person O, Person B, Wexner SD. Hemorrhoidal disease: A comprehensive review. J Am Coll Surg. 2007 Jan;204(1):102-17. Epub 2006 Oct 25.[pubmed]
22. Chaleoykitti B. Comparative study between multiple and single rubber band ligation in one session for bleeding internal, hemorrhoids: a prospective study. J Med Assoc Thai. 2002 Mar;85(3):345-50.[pubmed]
23. MacRae HM, McLeod RS. Comparison of hemorrhoidal treatment modalities. A meta-analysis. Dis Colon Rectum. 1995 Jul;38(7):687-94.[pubmed]
24. Lango A. Treatment of hemorroids disease by reduction of mucosa and hemorrhoidal prolapse with a circular stapler suturing device: A new procedure. In Proceeding of the 6th world Congress of Endoscopic Surgery. Rome, 3-6 June, 1998.
25. Burch J, Epstein D, Sari AB, et al. Stapled haemorrhoidopexy for the treatment of haemorrhoids: a systematic review. Colorectal Dis. 2009 Mar;11(3):233-43; discussion 243. doi: 10.1111/j.1463-1318.2008.01638.x.Epub 2008 Jul 15.[pubmed]

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





