
Clinico pathological study of right iliac fossa masses and their management
Abstract
Aim: The present study aims to study causes, modes of presentation, investigations of choice and management of right iliac fossa masses. Materials and
Methods: A prospective study was undertaken on 50 patients presenting with mass in right iliac fossa to surgery outpatient department during the period august 2015 to October 2017. All cases were investigated and managed as per protocol and their data recorded. All the demographic variables were tabulated as per percentage among total cases.
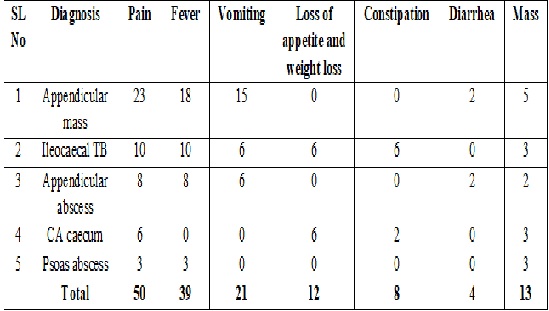
Results: In this series out of 50 patients, 23 patients (46%) diagnosed to have Appendicular mass followed by Ileocaecal TB (20%), Appendicular abscess (16%), CA Caecum (12%) and psoas abscess (6%). Appendicular pathology is more common in 3rd decade, Ileocaecal TB in 4thdecade, CA Caecum and Psoas abscess in 6th decade.In total of 50 patients, 28 (56%) were males and 22 (44%) were females. In the present study pain was the commonest symptom of presentation seen in all cases, fever was present in 78% cases, vomiting was present in 42% cases, loss of weight and appetite was present in 24% cases, constipation was present in 16% cases, diarrhea was present in 8% cases, mass per abdomen was present in 26% cases.
Conclusion: The common cause of right iliac fossa mass is of appendicular pathology followed by lleocaecal TB, Carcinoma caecum and psoas abscess in that order, with male preponderance and most of cases falling in 3rd decade.
Downloads
References
2. Dnyanmote AS, Sinha N, Chavan S, Sable S.Clinico pathological study of RIF mass. Web med central general Surgery 2014;5(11).
3. Carpenter SG, Chapital AB, Merritt MV, Johnson DJ. Increased risk of neoplasm in appendicitis treated with interval appendectomy: single-institution experience and literature review. Am Surg. 2012 Mar;78(3):339-43.[pubmed]
4. Furman MJ, Cahan M, Cohen P, Lambert LA. Increased risk of mucinous neoplasm of the appendix in adults undergoing interval appendectomy. JAMA Surg. 2013 Aug;148(8):703-6. doi: 10.1001/jamasurg.2013.1212.[pubmed]
5. Madhushankar L, Satish Kumar R, Sanjay SC. Roll of USG in preoperative evaluation of RIF mass. Journal of evolution of Medical and Dental sciences 2013;2(126):9030-36.
6. Richardson NG, Heriot AG, Kumar D, Joseph AE. Abdominal ultrasonography in the diagnosis of colonic cancer. Br J Surg. 1998 Apr;85(4):530-3. DOI:10.1046/j.1365-2168.1998.00637.x.[pubmed]
7. Teixeira PG, Demetriades D. Appendicitis: changing perspectives. Adv Surg. 2013;47:119-40.[pubmed]
8. Bakhshi G D, Deshpande S, Jadav K V, Shenoy SS, Yadav R. Abdominal kochs: An analysis – an Indian perspective . International journal of medical and applied sciences 2013;2(3):248-254.
9. Dutta gupta A. K., Intestinal tuberculosis, Indian journal of surgery,1958,20:396-400.
10. Bartolo DCC. psoas abscess in bristol – a 10 year review. Int. J. colorectal Dis., 1987,2:72-6.[pubmed]
11. Kedar RP, Shah PP, Shivde RS, Malde HM. Sonographic findings in gastrointestinal and peritoneal tuberculosis. Clin Radiol. 1994 Jan;49(1):24-9.[pubmed]
12. Lee DH, Ko YT, Yoon Y, Lim JH. Sonographic findings of intestinal tuberculosis. J Ultrasound Med. 1993 Sep;12(9):537-40.[pubmed]
13. Pettengelet al. Colonoscopic features of early tuberculosis – a report of 11 cases. S.AF.Med J, 1991, march .2:79(5):279-280.[pubmed]
14. Wall SD, Fisher MR, Amparo EG, et al. Magnetic resonance imaging in the evaluation of abscesses. AJR Am J Roentgenol. 1985 Jun;144(6):1217-21.[pubmed]
15. Bhansali S K. Abdominal Tuberculosis: A clinical analysis of 135 cases. Indian journal of surgery, 1968 ,30 :72-76.
16. Deelder JD, Richir MC, Schoorl T, Schreurs WH. How to treat an appendiceal inflammatory mass: operatively or nonoperatively? J Gastrointest Surg. 2014 Apr;18(4):641-5. doi: 10.1007/s11605-014-2460-1. Epub 2014 Feb 4.[pubmed]
17. Zhang HL, Bai YZ, Zhou X, Wang WL. Nonoperative management of appendiceal phlegmon or abscess with an appendicolith in children. J Gastrointest Surg. 2013 Apr;17(4):766-70. doi: 10.1007/s11605-013-2143-3. Epub 2013 Jan 12.[pubmed]
18. Thomas DR. Conservative management of the appendix mass. Surgery. 1973 May;73(5):677-80.[pubmed]
19. Anand S.S. Hypertrophic ileocaecal tuberculosis in India with a record of 50 Hemicolectomies. Annals of royal college of surgeons,1956,19:205-222.
20. Pujari BD. Modified surgical procedures in intestinal tuberculosis. Br J Surg. 1979 Mar;66(3):180-1.[pubmed]
21. Shashikala V et al / International Journal of Biomedical and Advance Research 2016; 7(8): 388-392.
22. S K Shetty, M Shankar. A Clinical Study Of Right Iliac Fossa Mass. The Internet Journal of Surgery. 2013 Volume 30 Number 4.
23. Bradley EL 3rd, Isaacs J. Appendiceal abscess revisited. Arch Surg. 1978 Feb;113(2):130-2.[pubmed]
24. Walsh TR, Reilly JR, Hanley E, et al. Changing etiology of iliopsoas abscess. Am J Surg. 1992 Apr;163(4):413-6.[pubmed]
25. Philip Abraham and Ferosh P. Mistry, “Tuberculosis of the Gastrointestinal Tract”, Ind J Pub,1992,39,251.
26. Prakash ATM. Intestinal tuberculosis - 10 years review. Indian Journal of surgery, 1978, Feb March; 56-65.
27. Prakash A, Sharma LK, Koshal A, et al. Ileocaecal tuberculosis. Aust N Z J Surg. 1975 Nov;45(4):371-5.[pubmed]
28. Bhansali, S.K. (1978) The challenge of abdominal tuberculosis in 310 cases. Ind. J. Surg., 40, No. 2 &3,65-77.
29. Prakash, Atm. (1978) Intestinal tuberculosis. 18 Year Review. Ind. J. Surg. Vol. 40, No. 2 & 3, p. 56-64.
30. Amin MA, Khan MA, Ayub M, et al. Delay in the diagnosis and prognosis of caecal carcinoma--a study of 20 cases. J Ayub Med Coll Abbottabad. 2001 Apr-Jun;13(2):28-31.[pubmed]
31. Mc Dermatt FT. Comparative results of surgical management of single carcinoma of the colon and rectum: a series of1939 patients managed by a single surgeon. Br J Surg, 1981; 68:850-855.
32. S K Shetty, M Shankar. A Clinical Study Of Right Iliac Fossa Mass. The Internet Journal of Surgery,2013,vol.30,no.4.
33. Goligher JC, Smiddy FG. The treatment of acute obstruction or perforation with carcinoma of colon and rectum. Br J Surg. 1957:270.[pubmed]
34. Gomez D, Dalai Z, Raw E, Roberts C, Lyndon PJ. Anatomical distribution of colorectal cancer over 10 year period in a district general hospital: is there a true rightward shift? Postgraduate Med J 2004;80:667-669.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





