
Peri-operative hyponatremia in orthopaedic injury patients
Abstract
Introduction: Hyponatremia is a common electrolyte disorder, particularly in orthopeadic trauma surgery patients and associated with adverse clinical outcomes. The aim of the study is to define the patient demographics, associated risk factors and clinical outcomes.
Methods: We evaluated patients admitted with major orthopeadic trauma in a tertiary care academic institution. Elderly patients morethan 65 years, who developed hyponatremia pre-operatively or post-operatively were included in the study. Basic demographic data, risk factors for, medication use, duration of hospital stay, in patient deaths were recorded.
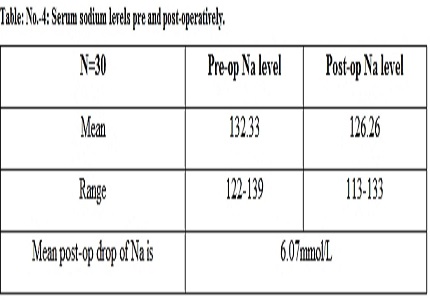
Results: Thirty patients were included. Mean age is 72.4 years. There were 20 females (66.6%). Risk factors (comorbidities) that cause hyponatremia were present in 73.3% (n=22). The most common comorbidities are hypertension 53.3% (n=16), DM 26.6% (n=8), CRF 16.6% (n=5), heart disease 16.6% (n=5). Drug induced hyponatemia is frequently caused by thiazide diuretics 20% (n=6) and anti-depressants 20% (n=6).The mean serum sodium pre-operatively 132.33 mmol/L (range 122-139) and mean post-op sodium level of 126.26 mmol/L (range 113-133) with mean post-op sodium level drop of 6.07 mmol/L. Twenty one patients had mild to moderate hyponatremia. The most frequent symptom was disorientation 40% (n=12), nausea and vomiting 26.6% (n=8), headache 10% (n=3) and seventeen percent (n=5) of the subjects were asymptomatic. The mean duration of hospital stay was 15.7 days (range 5-42 days), seven patients (23.3%) required ICU care and 2 patients (6.6%) died in the hospital.
Conclusion: The most common risk factors that cause hyponatremia are hypertension and diabetes. Diuretics and antidepressant drugs are common causative factors. Average decrease in serum sodium level post operatively should be expected in this age group. Majority had mild to moderate hyponatremia. Total length of the hospital stay (TLOS) is increased compared to normal discharge. Mortality rate is also higher.
Downloads
References
2. Beloosesky Y, Hershkovitz A, Solovey B, Salai M, Weiss A. Hip fracture post-operation dysnatremia and Na+ courses in different cognitive and functional patients groups. Arch GerontolGeriatr. 2011;53(2):179-182.https://doi.org/10.1016/j.archger.2010.10.014.
3. Hennrikus E., Ou, G., Kinney, B., Lehman, E., Grunfeld, R., Wieler, J., Damluji, A., Davis III, C. and Mets, B. Prevalence, Timing, Causes, and outcomes of Hyponatremia in HospilizedOrthopaedic Surgery Patients. J Bone Joint Surg Am. 2015 Nov 18;97(22):1824-32. doi: 10.2106/JBJS.O.00103. [PubMed]
4. Desborough JP. The stress response to trauma and surgery. BrJ Anaesth,1July2000;85(1);109–117,https://doi.org/10.1093/bja/85.1.109. [PubMed]
5. Tambe AA, Hill R, Livesley PJ. Post-operative hyponatraemia in orthopaedic injury. Injury. 2003 May;34(4):253-5. [PubMed]
6. Soiza RI., Hoyle GE, Chua MPW. Electrolyte and salt disturbances in older people: causes ,management and implications. Rev ClinGerontol,2008 18(2):143-158.
7. Ayus CJ, ArieffAI.Brain damage and post-operative hypnatremia;the role of gender. Neurology 1996; 46(2); 323-8. [PubMed]
8. Sandhu HS, Gilles E., De Vita MV, Panagopoulos G, Michelis MF. Hyponatremia associated with large bone fractures in elderly patients. IntUrolNephrol, 2009 ,41(3):733-737Doi 10.1007/s11255-009-9585-2.
9. Clayton JA, Le Jeune IR, Hall IP. Severe hyponatremia in medical inpatients. Aetiology, assessment and outcome. QJM 2006; 99(8): 505-511.https://doi.org/10.1093/qjmed/hcl071.
10. Bagshaw S, Townsend D, McDermid R. Disorders of sodium and water balance in hospitalized patients. Can J Anesth (2009) 56(2):151–167 DOI 10.1007/s12630-008-9017-2. [PubMed]
11. Robertson GL. Antidiuretic hormone. Normal and disordered function. Endocrinol MetabClin North Am. 2001 Sep;30(3):671-94, vii. [PubMed]
12. Henrikus E, Georgeson A, Ley meister K, Mucha S, Mc Gillen B, Miller R. Defining the cause of post-operative hyponatremia in the orthopeadic patient. International journal of clinical medicine 2016; 7, 668-674. DOI: 10.4236/ijcm.2016.710072.
13. Cumming K, Hoyle GE, Hutchison JD, SoizaRL.Prevalence, incidence and etiology of hyponatremia in elderly patients with fragility fractures. PLoS One. 2014 Feb 5;9(2):e88272. doi: 10.1371/journal.pone.0088272. eCollection 2014. [PubMed]
14. Liamis G, Milionis H, Elisaf M. A review of drug induced hyponatremia. Am J kidney Dis. 2008; 52(1): 144-153. DOI: http://dx.doi.org/10.1053/j.ajkd.2008.03.004. [PubMed]
15. Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Med. 2009 Sep;122(9):857-65. doi: 10.1016/j.amjmed.2009.01.027. [PubMed]

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





