
Prediction of difficult laparoscopic cholecystectomy while working up the patient for surgery
Abstract
Introduction: Laparoscopic cholecystectomy [LC] has established itself as standard of care for gallstone disease. With the wide availability of expertise, complication rate and conversion rate both are coming down. Coupled with increase in patient awareness and easy accessibility of information, it is becoming increasingly difficult for surgical team to explain complication arising following surgery. A preoperative prediction can help ease doctor-patient relationship.
Objective: To find out the predictors of difficult laparoscopic cholecystectomy while investigating the patient for surgery. Patient and methods: We selected 125 patients based on convenient sampling who underwent LC. A Likert type questionnaire was used to assess the difficulty. Weighted difficulty score [WDS] was calculated as the sum of product of parameter response and difficulty response score [WDS= ∑ (PR x DRS)]. Mean WDS was then compared against preoperative investigation findings.
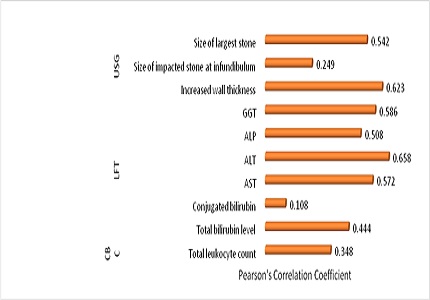
Results: Mean WDS was found to increase with raised leukocyte count as well as with altered liver function tests. Thickened gallbladder wall in ultrasonography had a positive correlation with difficulty in surgery but no association was found with the pericholecystic fluid. A larger size of stone, stone impacted at neck and a larger size of the impacted stone were all had a significant positive association with difficult LC but number of stones in GB had no impact on difficulty during surgery in our study. Altered liver echotexture and a contracted GB were the other factors which can predict a possible difficulty during LC.
Conclusion: A careful watch on investigation which include leukocyte count, liver function tests and preoperative ultrasonography can help predict the difficulty, a possibility of conversion as well as complications. A discussion of these events with the patients and their relatives can create an atmosphere of mutual trust and better prepare to overcome of untoward events.
Downloads
References
2. Jackson PG, Evans SRT. Biliary system. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. Sabiston textbook of Surgery, the biological basis of modern surgical practice. 20th edition. Philadelphia: Elsevier. 2017. 1482.
3. Kotwal MR, Rinchen CZ. Gallstone disease in the Himalayas (Sikkim and north Bengal): causation and stone analysis. Indian J Gastroenterol. 1998 Jul-Sep;17(3):87-9. [PubMed]
4. Kharga B, Sharma BK, Singh VK, Nishant K, Bhutia P, Tamang R et al. Obesity not necessary, risk of symptomatic cholelithiasis increases as a function of BMI. JCDR. 2016;10(10):PC28-32. DOI: 10.7860/JCDR/2016/22098.8736.
5. KumarS, Tiwary S, Agrawal N, Prasanna G, Khanna R, Khanna A: Predictive Factors for Difficult Surgery in Laparoscopic C holecystectomy for C hronic C holecystitis. The Internet Journal of Surgery. 2008;16(2). DOI: 10.5580/154e.
6. Yetkin G, Uludag M, Citgez B, Akgun I, Karakoc S.Predictivefactors for conversion of laparoscopic cholecystectomy in patients with acute cholecystitis. Bratisl Lek Listy. 2009;110(11):688-91. [PubMed]
7. Lipman JM, Claridge JA, Haridas M, Martin MD, Yao DC, Grimes KL, Malangoni MA. Preoperative findings predict conversion from laparoscopic to open cholecystectomy. Surgery. 2007 Oct;142(4):556-63; discussion 563-5. [PubMed]
8. Rosen M, Brody F, Ponsky J. Predictive factors for conversion of laparoscopic cholecystectomy. Am J Surg. 2002 Sep;184(3):254-8. [PubMed]
9. Vivek MAKM, Augustine AJ, Rao R: A comprehensive predictive scoring method for difficult laparoscopic cholecystectomy. Journal of Minimal Access Surgery. 2014; 10:2.DOI: 10.4103/0972-9941.129947.
10. Polychronidis A, Botaitis S, Tsaroucha A, et al. Laparoscopic Cholecystectomy in Elderly Patients. J Gastrointestin Liver Dis. 2008;17(3):309-313. [PubMed]
11. Alponat A, Kum CK, Koh BC, Rajnakova A, Goh PM. Predictive factors for conversion of laparoscopic cholecystectomy. World JSurg. 1997 Jul-Aug;21(6):629-33. [PubMed]
12. Kama NA, Kologlu M, Doganay M, Reis E, Atli M, Dolapci M. A risk score for conversion from laparoscopic to open cholecystectomy. Am J Surg. 2001 Jun;181(6):520-5. [PubMed]
13. Lal P, Agarwal PN, Malik VK, Chakravarti AL. A difficultlaparoscopic cholecystectomy that requiresconversion to openprocedure can be predicted by preoperativeultrasonography. JSLS. 2002 Jan-Mar;6(1):59-63. [PubMed]
14. Nachnani J, Supe A. Pre-operative prediction of difficult laparoscopic cholecystectomy using clinical and ultra-sonographic parameters. Indian J Gastroenterol. 2005 Jan-Feb;24(1):16-8.
15. Nachnani J, Supe A. Pre-operative prediction of difficult laparoscopic cholecystectomy using clinical and ultrasonographic parameters. Indian J Gastroenterol. 2005 Jan-Feb;24(1):16-8.
16. Gholipour C, Fakhree MBA, Shalchi RA, Abbasi M. Prediction of conversion of laparoscopic cholecystectomy to open surgery with artificial neural networks. BMC Surgery. 2009; 9:13, DOI:10.1186/1471-2482-9-13.
17. Morino M, Cavuoti G, Miglietta C, Giraudo G, Simone P.Laparoscopic cholecystectomy in cirrhosis: contraindication or privilegedindication?Surg Laparosc Endosc Percutan Tech. 2000 Dec;10(6):360-3.
18. Shaikh AR, Muneer A. Laparoscopic cholecystectomy in cirrhotic patients. JSLS. 2009 Oct-Dec;13(4):592-6. doi: 10.4293/108680809X12589999537959.
19. Laurence JM, Tran PD, Richardson AJ, Pleass HC, Lam VW. Laparoscopic or open cholecystectomy in cirrhosis: a systematic review of outcomes and meta-analysis of randomized trials. HPB (Oxford). 2012 Mar;14(3):153-61. doi: 10.1111/j.1477-2574.2011.00425.x. Epub 2012 Jan 18.
20. Jansen S, Jorgensen J, Caplehorn J, Hunt D.Preoperativeultrasound to predict conversion in laparoscopic cholecystectomy. Surg Laparosc Endosc.1997Apr;7(2):121-3. [PubMed]
21. Fried GM, Barkun JS, Sigman HH, Joseph L, Clas D, Garzon J, Hinchey EJ, Meakins JL.Factorsdeterminingconversion to laparotomy in patientsundergoinglaparoscopic cholecystectomy. Am J Surg. 1994 Jan;167(1):35-9; discussion 39-41. [PubMed]

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





