
Silent but Serious: A Case of Colonic Perforation Masquerading as a Persistent Retrorectus Abscess Post Blunt Abdominal Trauma
Abstract
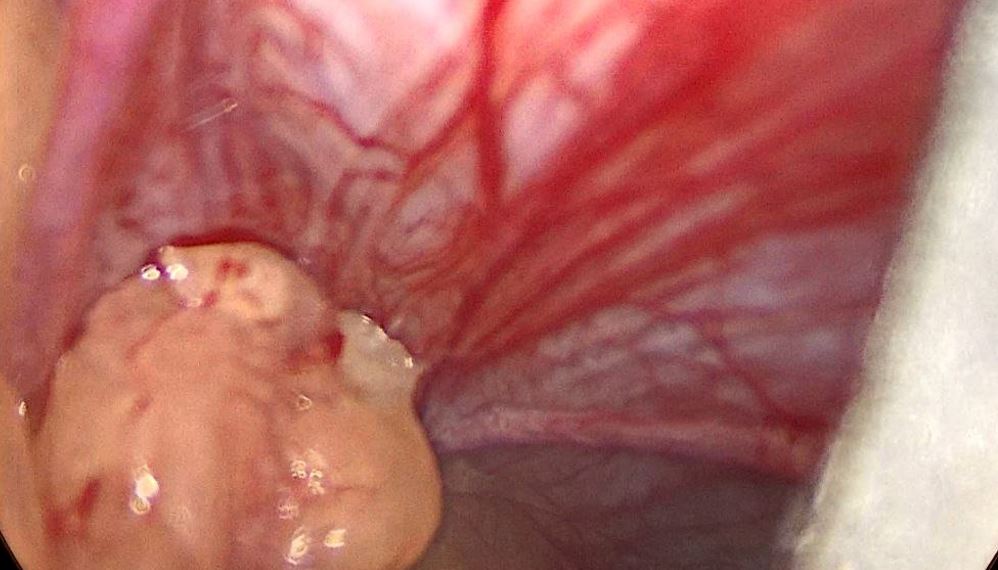
A 21-year-old male presented with fever and abdominal pain 10 days after a minor fall. Imaging revealed pelvic abscess and possible hollow viscus perforation. Laparoscopy identified adhesion of omentum and sigmoid colon with abdominal wall covering a defect of 2x2 with 600 ml pus collection in extra peritoneal retro rectus space necessitating laparotomy. No bowel injury identified, and the patient initially improved. However persistent purulent discharge led to a repeat CECT revealing loculated abscess with air tracking to the skin. Re-exploration revealed sealed colonic perforation. Managed conservatively for a low output enterocutaneous fistula, showed significant improvement.
Downloads
References
2. Bruscagin V1 et al. Blunt gastric injury. A multicentre experience. Injury. 2001;32(10):761-4.]
3. Fakhry SM, et al. EAST Multi-Institutional Hollow Viscus Injury Research Group. Current diagnostic approaches lack sensitivity in the diagnosis of perforated blunt small bowel injury: analysis from 275,557 trauma admissions from the EAST multi-institutional HVI trial. J Trauma. Acute Care Surg 2003 Feb;54(2):295-306.
4. Hamidian Jahromi A, et al. Delayed small bowel perforation following blunt abdominal trauma: A case report and review of the literature. Asian J Surg. 2016 Apr;39(2):109-12.
5. Fakhry SM, Brownstein M, Watts DD,Baker CC, Oller D. Relatively short diagnostic delays (<8 hours) produce morbidity and mortality in blunt small bowel injury: an analysis of time tooperative intervention in 198 patients From a multicenter experience. J Trauma. 2000;48(3):408-14.].
6. Jha NK, et al. Characteristics of Hollow Viscus Injury following Blunt Abdominal Trauma; a Single Centre Experience from Eastern India. Bull Emerg Trauma. 2014;2(4):156-160.
7. Ertugrul et al. Delayed presentation of a sigmoid colon injury following blunt abdominal trauma: a case report. Journal of Medical Case Reports 2012 6:247.
8. Chophel T et al. Jejunal perforation after a trivial trauma: A case report. SAGE Open Med Case Rep. 2022 Jul 7;10:2050313X221110032.
9. Okello M, Batte C and Buwembo W. Jejunal transection following trivial trauma: case report and review of literature. IntJ Surg Case Rep 2016; 27: 41–43.
10. Sandiford NA, Sutcliffe RP and Khawaja HT. Jejunal tran-section after blunt abdominal trauma: a report of two cases.Emerg Med J 2006; 23(10): e55.]
11. Tirkes T, Sandrasegaran K, Patel AA, et al. Peritoneal and retroperitoneal anatomy and its relevance for cross-sectional imaging. Radiographics. 2012;32(2): 437-451.
12. Gore RM, Balfe DM, Aizenstein RI, Silverman PM. The great escape: interfascial decompression planes of the retroperitoneum. American Journal of Roentgenology. 2000; 175(2):363-370.]
13. Meyers M. The Extraperitoneal Spaces: Normal and Physiologic Anatomy. In: Dynamic Radiology of the Abdomen: Normal and Pathologic Anatomy, 6th Edition. Springer-Verlag New York. 2005
14. Matsui Y, Oikawa S, Sorimachi K, et al. Association of impact velocity with risks of serious injuries and fatalities to pedes- trians in commercial truck-pedestrian accidents. Stapp Car Crash J 2016; 60: 165–182]
15. Ricciardi R, Paterson CA, Islam S, Sweeney WB, Baker SP, Counihan TC: Independent predictors of morbidity and mortality in blunt colon trauma. Am Surg 2004, 70:75–79.]
Copyright (c) 2025 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





