
A characteristic of hollow viscus injury (HVI) following blunt abdominal trauma: a study done in Vandana Nursing Home and IVF Clinic, Hazaribag, Jharkhand, India
Abstract
Objective: To determine the presentation, anatomical distribution, diagnostic method, management and outcome of hollow viscus injury (HVI) from blunt abdominal trauma.
Methods: This was a retrospective cross-sectional study including patients with blunt abdominal trauma leading to HVI admitted at Vandana Nursing Home and IVF Clinic, Hazaribag. A prospective comparison study over a period of 6 years (April 2012 to May 2018). Data were retrieved from patients’ medical records. Total 43 patients with HVI due to blunt abdominal trauma, who underwent laparotomy at our institute, were reviewed. Data regarding clinical presentation, anatomical distribution, management and outcome were recorded and analysed.
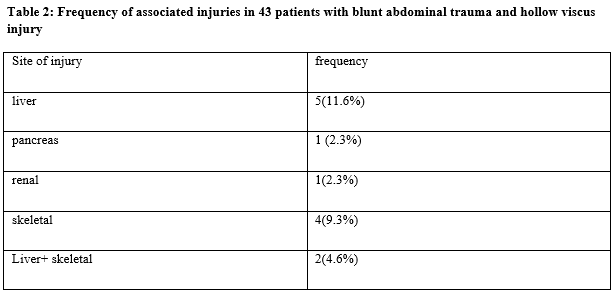
Results: Out of 43 patients 87.1% were men and 12.9% were women. Mean age of patients was 29±14.02 years. The most common site of injury was ileum (46.2%) followed by jejunum (44.5%). There were 2 gastric perforations (4.6%), 1 (2.3%) duodenal, 1 (2.3%) colonic, 1 (2.3%) sigmoidal and 1 (2.3%) rectal injuries. One caecal injuries was also recorded. Road traffic accident was the most common mechanism of injury (57.2%) followed by fall from height (36.4%) and assault (6.4%). Free gas under diaphragm on erect abdomen radiography was seen in 85.5% of cases while preoperative CT Abdomen was done in 11.6% of cases. Treatment consisted of simple closure of the perforation (66.5%), resection and anastomosis (11.0%) and stoma (22.5%). Major complication was anastamotic leak which was recorded in 6.4% cases and 15.6% patients developed burst abdomen. Average hospital stay was 13±6 days. Overall mortality rate was 12.7%.
Conclusion: Although early recognition of intestinal injuries from blunt abdominal trauma may be difficult in all cases, it is very important due to its tremendous life-threatening potential. Age of the patient, anatomical site and time of presentation are probably main prognostic factors
Downloads
References
Trauma Register DGU (®). 20 years of trauma documentation in Germany Actual trends and developments. Injury. 2014;45(3):S14-S9. doi: https://doi.org/10.1016/j.injury.2014.08.012.
Fakhry SM, Brownstein M, Watts DD, Baker CC, Oller D. Relatively short diagnostic delays (<8 hours) procedure morbidity and mortality in blunt small bowel injury: an analysis of time to operative intervention in 198 patients from a multicenter experience. J Trauma. 2000;48(3):408-414. doi: https://doi.org/10.1097/00005373-200003000-00007.
Bruscagin V, Coimbra R, Rasslan S, Abrantes WL, Souza HP, Neto G, et al. Blunt gastric injury.A multicentre from a multicenter experience.J Trauma. 2000;48(3):408-414. doi: https://doi.org/10.1016/s0020-1383(01)00081-x.
Magu S, Agarwal S, Gill RS. Multi detector computed tomography in the diagnosis of bowel injury. Indian J Surg. 2012;74(6):445-450. doi: https://dx.doi.org/10.1007%2Fs12262-011-0405-4.
Swaid F, Peleg K, Alfici R, Matter I, Olsha O, Ashkenazi I, et al. Concomitant hollow viscus injuries in patients with blunt hepatic and splenic injuries: An analysis of a National Trauma Registry database. Injury. 2014;45(9):1409-1412. doi: https://doi.org/10.1016/j.injury.2014.02.027.
Abbasi HR, Mousavi SM, Taheri Akeri A, Niakan MH, Bolandparvaz S, Paydar S. Pattern of Traumatic Injuries and Injury Severity Score in a Major Trauma Center in Shiraz, Southern Iran. Bull Emerg Trauma. 2013;1(2):81-85.
Pekkari P, Bylund PO, Lindgren H, Öman M. Abdominal injuries in a low trauma volume hospital--a descriptive study from northern Sweden. Scand J Trauma Resusc Emerg Med. 2014;22:48. doi: https://doi.org/10.1186/s13049-014-0048-0.
Arikanoglu Z, Turkoglu A, Taskesen F, Ulger BV, Uslukaya O, Basol O, et al. Factors affecting morbidity and mortality in hollow visceral injuries following blunt abdominal trauma. Clin Ter. 2014;165(1):23-26. doi: https://doi.org/10.7417/CT.2013.1656.
Matsushima K, Mangel PS, Schaefer EW, Frankel HL. Blunt hollow viscus and mesenteric injury: still underrecognized. World J Surg. 2013;37(4):759-765. doi: https://doi.org/10.1007/s00268-012-1896-2.
Gonser-Hafertepen LN, Davis JW, Bilello JF, Ballow SL, Sue LP, Cagle KM, et al. Isolated free fluid on abdominal computed tomography in blunt trauma: watch and wait or operate? J Am Coll Surg. 2014;219(4):599-605. doi: https://doi.org/10.1016/j.jamcollsurg.2014.04.020.
Watts DD, Fakhry SM; EAST Multi-Institutional Hollow Viscus Injury Research Group. Incidence of hollow viscus injury in blunt trauma: an analysis from 275,557 trauma admissions from the East multi-institutional trial. J Trauma. 2003;54(2):289-294. doi: https://doi.org/10.1097/01.TA.0000046261.06976.6A.
Kulvatunyou N, Albrecht RM, Bender JS, Friese RS, Joseph B, Latifi R, et al. Seatbelt triad: severe abdominal wall disruption, hollow viscus injury, and major vascular injury. Am Surg. 2011;77(5):534-538.
Kane NM, Francis IR, Burney RE, Wheatley MJ, Ellis JH, Korobkin M. Traumatic pneumoperitoneum. Implications of computed tomography diagnosis. Invest Radiol. 1991;26(6):574-578.
Chirdan LB, Uba AF, Chirdan OO. Gastrointestinal injuries following blunt abdominal trauma in children. Niger J Clin Pract. 2008;11(3):250-253.
Ameh EA, Nmadu PT. Gastrointestinal injuries from blunt abdominal trauma in children. East Afr Med J. 2004;81(4):194-197. doi: https://doi.org/10.4314/eamj.v81i4.9154.
Sule AZ, Kidmas AT, Awani K, Uba F, Misauno M. Gastrointestinal perforation following blunt abdominal trauma. East Afr Med J. 2007;84(9):429-433. doi: https://doi.org/10.4314/eamj.v84i9.9552.
Khan I, Bew D, Elias DA, Lewis D, Meacock LM. Mechanisms of injury and CT findings in bowel and mesenteric trauma.Clin Radiol. 2014;69(6):639-647. doi: https://doi.org/10.1016/j.crad.2014.01.021.
Fraga GP, Silva FH, Almeida NA, Curi JC, Mantovani M. Blunt abdominal trauma with small bowel injury: are isolated lesions riskier than associated lesions? Acta Cir Bras. 2008;23(2):192-197. doi: https://doi.org/10.1590/s0102-86502008000200013.
Nural MS, Yardan T, Güven H, Baydin A, Bayrak IK, Kati C. Diagnostic value of ultrasonography in the evaluation of blunt abdominal trauma. Diagn Interv Radiol. 2005;11(1):41-44.
Killeen KL, Shanmuganathan K, Poletti PA, Cooper C, Mirvis SE. Helical computed tomography of bowel and mesenteric injuries. J Trauma. 2001;51(1):26-36. doi: https://doi.org/10.1097/00005373-200107000-00005.
Miller LA, Shanmuganathan K. Multidetector CT evaluation of abdominal trauma. Radiol Clin North Am. 2005;43(6):1079-1095. doi: https://doi.org/10.1016/j.rcl.2005.08.007.
Scaglione M, de Lutio di Castelguidone E, Scialpi M, Merola S, Diettrich AI, Lombardo P, et al. Blunt trauma to the gastrointestinal tract and mesentery: is there a role for helical CT in the decision-making process? Eur J Radiol. 2004;50(1):67-73. doi: https://doi.org/10.1016/j.ejrad.2003.11.016.
Lawson C, Daley BJ, Ormsby CD, Enderson B. Missed injuries in the era of the trauma scan. J Trauma. 2011;70(2):452-456. doi: https://doi.org/10.1097/TA.0b013e3182028d71.
Curran TJ, Borzotta AP. Complications of primary repair of colon injury: literature review of 2964 cases. Am J Surg. 1999;177(1):42-47. doi: https://doi.org/10.1016/s0002-9610(98)00293-1.
Burch JM. Injury to the colon and rectum. In: Moore EE, Feliciano DV, Mattox KL (eds) Trauma, 5th ed. McGraw Hill, New York; 2004. p. 735-753.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





