
Analysis of surgical management and outcome of Blunt abdominal trauma
Abstract
Background: Trauma, in particular, blunt abdominal trauma, associated with vehicular accidents and railway accident, has become major cause of morbidity and mortality for working population in developing and industrial nations of world. Hence the present study was undertaken to assess the surgical management and outcome of Blunt abdominal trauma.
Method: 49 cases of blunt abdominal trauma studied during study period in a tertiary care hospital. On admission a relevant history with nature of accident, time of occurrence and injuries sustained were noted. A detailed examination of the patient was done, which included general examination with appropriate recording of pulse, blood pressure, and respiratory rate at time of admission, and systemic examination of chest abdomen and central nervous system. Details of external, skeletal and other associated injuries were noted. Presence or absence of hematuria was also recorded.
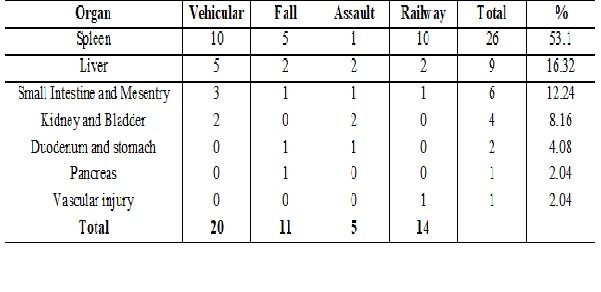
Result: Predominantly younger population (21-30) is affected by trauma with male (10-1) preponderance. Vehicular accident was the commonest cause (48.4%). Blind abdominal tap was 53% sensitive for hemoperitoneum while USG 90%. CT was almost 100% sensitive for abdominal injuries. Spleen (53.08%) and liver (22.44%) were the common organs injured. Associated injuries were present in 42.85% cases. Mortality was higher in those operated beyond one hour.
Conclusion: Prevention and measures to decrease morbidity and mortality from abdominal trauma is essential to avoid loss of productive years of life. Trauma registry with documentation of care delivered, assessment of outcome and implementation of necessary changes would help in providing better care.
Downloads
References
2. Shuck JM, Lowe RJ. Intestinal disruption due to blunt abdominal trauma. Am J Surg. 1978 Dec;136(6):668-73.[pubmed]
3. Munns J, Richardson M, Hewett P. A review of intestinal injury from blunt abdominal trauma. Aust N Z J Surg. 1995 Dec;65(12):857-60.[pubmed]
4. Guirguis EM, Hong C, Liu D, et al. Trauma outcome analysis of two Canadian centres using the TRISS method. J Trauma. 1990 Apr;30(4):426-9.[pubmed]
5. Rhodes M, Aronson J, Moerkirk G, et al. Quality of life after the trauma center. J Trauma. 1988 Jul;28 (7):931-8.[pubmed]
6. Kreis JD, Fine EG, Gomez GA, Eckes JE, Whitwell EN, Byers PM. A prospective evaluation of field categorization of trauma patients. The Journal of trauma. 1988 Jul;28(7):995-1000.[pubmed]
7. Sayers RD, Bewes PC, Porter KM. Emergency laparotomy for abdominal trauma. Injury. 1992;23(8):537-41.[pubmed]
8. Eastman A. The formation, isolation and characterization of DNA adducts produced by anticancer platinum complexes. Pharmacol Ther. 1987;34(2):155-66.[pubmed]
9. Blow O, Magliore L, Claridge JA, et al. The golden hour and the silver day: detection and correction of occult hypoperfusion within 24 hours improves outcome from major trauma. J Trauma. 1999 Nov;47(5):964-9.[pubmed]
10. Gupta S, Talwar S, Sharma RK, et al. Blunt trauma abdomen: a study of 63 cases. Indian J Med Sci. 1996 Aug;50(8):272-6.[pubmed]
11. Oreskovithch MR, Carrico E. Management of acutely injured patients. Textbook of surgery. Vol 1. Philadelphia lgakustrion / Saunders. 1986; 17: 294 – 299.[pubmed]
12. Nast-Kolb D, Waydhas C, Kastl S, et al. [The role of an abdominal injury in follow-up of polytrauma patients]. Chirurg. 1993 Jul;64(7):552-9.[pubmed]
13. Fakhry SM, Brownstein M, Watts DD, et al. Relatively short diagnostic delays (<8 hours) produce morbidity and mortality in blunt small bowel injury: an analysis of time to operative intervention in 198 patients from a multicenter experience. J Trauma. 2000 Mar;48(3):408-14; discussion 414-5.[pubmed]
14. Clarke JR, Trooskin SZ, Doshi PJ, et al. Time to laparotomy for intra-abdominal bleeding from trauma does affect survival for delays up to 90 minutes. J Trauma. 2002 Mar;52(3):420-5.[pubmed]
15. Shweiki E, Klena J, Wood GC, et al. Assessing the true risk of abdominal solid organ injury in hospitalized rib fracture patients. J Trauma. 2001 Apr;50(4):684-8.[pubmed]
16. Moore EE, Malangoni MA, Cogbill TH, et al. Organ injury scaling. IV: Thoracic vascular, lung, cardiac, and diaphragm. J Trauma. 1994 Mar;36(3):299-300.[pubmed]
17. Abu-Zidan FM, Sheikh M, Jadallah F, et al. Blunt abdominal trauma: comparison of ultrasonography and computed tomography in a district general hospital. Australas Radiol. 1999 Nov;43(4):440-3.[pubmed]
18. Brown MA, Casola G, Sirlin CB, et al. Blunt abdominal trauma: screening us in 2,693 patients. Radiology. 2001 Feb;218(2):352-8. DOI:10.1148/radiology.218.2.r01fe42352.[pubmed]
19. Ballard RB, Rozycki GS, Newman PG, et al. An algorithm to reduce the incidence of false-negative FAST examinations in patients at high risk for occult injury. Focused Assessment for the Sonographic Examination of the Trauma patient. J Am Coll Surg. 1999 Aug;189(2):145-50; discussion 150-1.[pubmed]

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





