Silent but Serious: A Case of Colonic Perforation Masquerading as a Persistent Retrorectus Abscess Post Blunt Abdominal Trauma
Saurabh A1, Sivastava NK2, Gond AK3*, Kushwaha P4, Kumar S5
DOI:https://doi.org/10.17511/ijoso.2025.i01.01
1 Amritanshu Saurabh, Assistant Professor, General Surgery, All India Institute of Medical Sciences, Raebareli, UP, India.
2 Niraj Kumar Sivastava, Additional Professor, General Surgery, All India Institute of Medical Sciences, Raebareli, UP, India.
3* Ajay Kumar Gond, Junior Resident, General Surgery, All India Institute of Medical Sciences, Raebareli, UP, India.
4 Pranabh Kushwaha, Associate Professor, General Surgery, All India Institute of Medical Sciences, Raebareli, UP, India.
5 Shirish Kumar, Assistant Professor, General Surgery, All India Institute of Medical Sciences, Raebareli, UP, India.
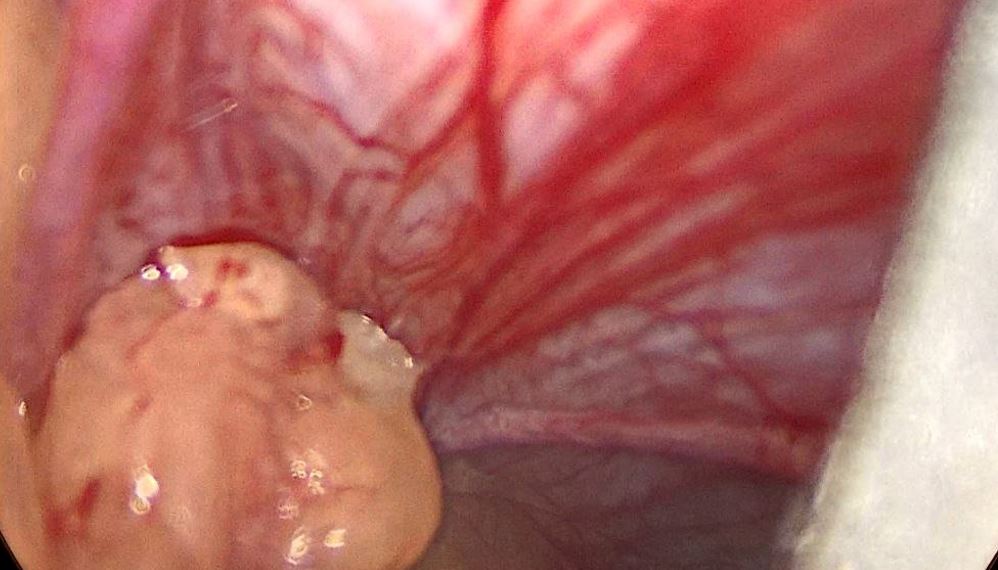
A 21-year-old male presented with fever and abdominal pain 10 days after a minor fall. Imaging revealed a pelvic abscess and possible hollow viscus perforation. Laparoscopy identified adhesion of omentum and sigmoid colon with abdominal wall covering a defect of 2x2 with 600 ml of pus collection in the extra peritoneal retro rectus space necessitating laparotomy. No bowel injury was identified, and the patient initially improved. However, persistent purulent discharge led to a repeat CECT revealing a loculated abscess with air tracking to the skin. Re-exploration revealed sealed colonic perforation. Managed conservatively for a low-output enterocutaneous fistula, showed significant improvement.
Keywords: Blunt abdominal trauma, retrorectus abscess, hollow viscus perforation, delayed complication, colonic perforation, enterocutaneous fistula
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Junior Resident, General Surgery, All India Institute of Medical Sciences, Raebareli, UP, India. Email:  |
Saurabh A, Sivastava NK, Gond AK, Kushwaha P, Kumar S, Silent but Serious: A Case of Colonic Perforation Masquerading as a Persistent Retrorectus Abscess Post Blunt Abdominal Trauma. Surgical Rev Int J Surg Trauma Orthoped. 2025;11(1):1-4. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/283 |
 |
 ©
©