Masquelet technique to treat a septic nonunion after plating of a femoral open fracture
Patel M.1*, Patel G.2, Chaudhary J.3, Patel A.4, Joshi M.5
DOI: https://doi.org/10.17511/ijoso.2023.i02.01
1* Maulik Patel, DNB Ortho Resident, Diploma in Orthopaedics, GMERS medical college and Hospital, Dharpur, Patan, Gujrat, India.
2 Gaurang Patel, Associate Professor, MS Orthopaedics, SSG Hospital and Medical College, Baroda, Vadodara, Gujrat, India.
3 Jaydeep Chaudhary, Senior Resident, MS Orthopaedics, GMERS medical college and hospital, Dharpur, Patan, Gujrat, India.
4 Abhay Patel, Junior Resident, Diploma in Orthopaedics, GMERS medical college and hospital, Dharpur, Patan, Gujrat, India.
5 Mayur Joshi, DNB Ortho Resident, Diploma in Orthopaedics, GMERS medical college and hospital, Dharpur, Patan, Gujrat, India.
Septic nonunion is one of the most common complications after an open fracture. The risk of infection and bony defects is high following an open fracture , and it is essential to address both issues to improve patient outcomes. Treatment can be complex and costly , and outcome is often uncertain. In the 1980s, Masquelet first described the induced membrane technique and autologous bone grafting to manage critical-size bone defects. In cases of Septic non-union, two different surgical steps are required for management. In the former step, radical management to control infection and in the latter step, biological stimulus to promote bone healing. In this case, we present a 28 years old female patient with an open grade 3A Femoral shaft Fracture. Initially , the patient received wound debridement and Femur plating which unfortunately resulted in septic non-union. Subsequently, the patient was managed with the induced membrane technique and a double-plate osteosynthesis to protect the biological chamber.
Keywords: Septic Nonunion, Masquelet Technique, Femoral Open Fracture
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , DNB Ortho Resident, Diploma in Orthopaedics, GMERS medical college and Hospital, Dharpur, Patan, Gujrat, India. Email:  |
Maulik Patel, Gaurang Patel, Jaydeep Chaudhary, Abhay Patel, Mayur Joshi, Masquelet technique to treat a septic nonunion after plating of a femoral open fracture. Surgical Rev Int J Surg Trauma Orthoped. 2023;9(2):6-12. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/270 |
 |
 ©
©  Figure 1 : X ray of right femur at the time of presentation .No callus formation at femur fracture end with visible sclerotic femur fracture end.
Figure 1 : X ray of right femur at the time of presentation .No callus formation at femur fracture end with visible sclerotic femur fracture end. Figure 2 : 2A & 2B- Fracture temporary stabilise with mon-axial external fixator.
Figure 2 : 2A & 2B- Fracture temporary stabilise with mon-axial external fixator.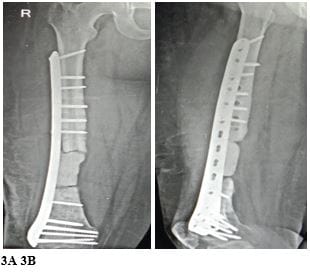 Figure 3 ( 3A & 3B ) : Antibiotic loaded cement space positioned together with distal femur plating.
Figure 3 ( 3A & 3B ) : Antibiotic loaded cement space positioned together with distal femur plating.
 Figure 5 ( 5A & 5B ) : X rays at one month follow up.
Figure 5 ( 5A & 5B ) : X rays at one month follow up. Figure 6 ( 6A & 6B ) : X rays at six months follow up showed complete graft integration as well as bony union.
Figure 6 ( 6A & 6B ) : X rays at six months follow up showed complete graft integration as well as bony union.