Case Report: An Unusual Location of Osteochondroma Dorsal Scapula
Patel M.1*, Parmar R.2, Modi P.3
DOI: https://doi.org/10.17511/ijoso.2023.i01.01
1* Maulik Patel, Diploma in Orthopaedics, DNB ortho Resident, GMERS medical college and Hospital, Dharpur, Patan, Gujrat, India.
2 Ruchir Parmar, MS Orthopaedics, Senior Resident, GMERS medical college and Hospital, Dharpur, Patan, Gujrat, India.
3 Pulkit Modi, MS Orthopaedics, Head of Department, GMERS medical college and Hospital, Dharpur, Patan, Gujrat, India.
Introduction: Osteochondroma of the scapula is one of the rare tumours of the thorax. It constitutes 14.4% of all tumours of the scapula with the ventral surface being the most common site of presentation. Based on our review of the literature, the dorsal surface of the scapula is a rare site of origin of osteochondroma. Among the osteochondroma of the dorsal surface of the scapula, the sessile variant is more common. Case Report: We reported a rare case of a solitary pedunculated variety of osteochondroma at an unusual site-dorsal surface of the scapula in a 9-year-old male child. The tumours were excised and the diagnosis was confirmed by histopathology. Conclusion: This case is reported for its rarity and unusual site of presentation.
Keywords: Scapula, osteochondroma, dorsal surface
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Diploma in Orthopaedics, DNB ortho Resident, GMERS medical college and Hospital, Dharpur, Patan, Gujrat, India. Email:  |
Maulik Patel, Ruchir Parmar, Pulkit Modi, Case Report: An Unusual Location of Osteochondroma Dorsal Scapula. Surgical Rev Int J Surg Trauma Orthoped. 2023;9(1):1-5. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/266 |
 |
 ©
©  Figure 1: Clinical Pre-operative Pictures (A hard, oval solid palpable mass on the dorsal scapula.)
Figure 1: Clinical Pre-operative Pictures (A hard, oval solid palpable mass on the dorsal scapula.) Figure 2: X-ray showing bony mass arising from the dorsal aspect of the scapula.
Figure 2: X-ray showing bony mass arising from the dorsal aspect of the scapula.
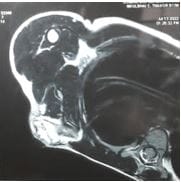
 Figure 3: MRI showing a pedunculated mass on the dorsal aspect of the scapula.
Figure 3: MRI showing a pedunculated mass on the dorsal aspect of the scapula. Figure 4: Intra-operative appearance of scapular osteochondroma.
Figure 4: Intra-operative appearance of scapular osteochondroma.  Figure 5: Pedunculated excised mass Figure 6: Post-excision local site.
Figure 5: Pedunculated excised mass Figure 6: Post-excision local site.