Incidental Finding of Pseudo Aneurysm of Superficial Femoral Artery and Severe Life-Threatening Bleeding from it During Revision Surgery for Failed Implant: A Case Report
Bisoniya H.1, Varma K.2*, Agarwal S.3, Sharma S.4
DOI: https://doi.org/10.17511/ijoso.2022.i06.01
1 H.S. Bisoniya, Consultant, Plastic and Vascular Surgeon, Bhopal Fracture Hospital, Bhopal, Madhya Pradesh, India.
2* K K Varma, Consultant, Orthopaedics and Director, Bhopal Fracture Hospital, Bhopal, Madhya Pradesh, India.
3 Shashank Agarwal, Consultant, Orthopaedics and Director, Bhopal Fracture Hospital, Bhopal, Madhya Pradesh, India.
4 Sandeep Sharma, Consultant, Orthopaedics and Director, Bhopal Fracture Hospital, Bhopal, Madhya Pradesh, India.
Arterial pseudoaneurysm formation is a rare entity following elective and trauma orthopaedic surgery. Pseudoaneurysms have been reported to occur following total knee arthroplasty, synovectomy and arthroscopic procedures. Here we report a case in which we encountered heavy bleeding while reoperating a case of the broken plate from the operated # shaft femur. On exploration, it was found that there was a pseudoaneurysm in the femoral artery size of rent 3mm, which probably was formed in his first surgery, which incidentally gave way and bled profusely.
Keywords: Pseudoaneurysms, synovectomy, arthroscopic procedures, heavy bleeding, reoperation
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Consultant, Orthopaedics and Director, Bhopal Fracture Hospital, Bhopal, Madhya Pradesh, India. Email:  |
H.S. Bisoniya, K K Varma, Shashank Agarwal, Sandeep Sharma, Incidental Finding of Pseudo Aneurysm of Superficial Femoral Artery and Severe Life-Threatening Bleeding from it During Revision Surgery for Failed Implant: A Case Report. Surgical Rev Int J Surg Trauma Orthoped. 2022;8(6):29-34. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/263 |
 |
 ©
©  Figure 1: X-Ray of the patient after the accident
Figure 1: X-Ray of the patient after the accident

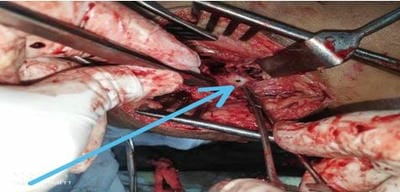
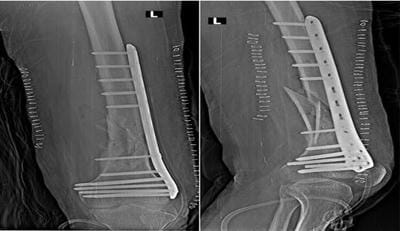 Fig 5: X-ray of the patient after revision surgery
Fig 5: X-ray of the patient after revision surgery