TB spine at the level of lumbosacral junction ( L5-S1 Level ): A Case report
Patel M.1*, Parmar R.2, Vala M.3, Modi P.4
DOI: https://doi.org/10.17511/ijoso.2022.i06.02
1* Maulik Patel, Diploma in Orthopaedics, DNB Ortho Resident, GMERS medical college and Hospital, Dharpur, Patan, Gujarat, India.
2 Ruchir Parmar, MS Orthopaedics, Senior Resident, GMERS medical college and Hospital, Dharpur, Patan, Gujarat, India.
3 Mayur Vala, MS Orthopaedics, Senior Resident, GMERS medical college and Hospital, Dharpur, Patan, Gujarat, India.
4 Pulkit Modi, MS Orthopaedics, Head of Department, GMERS medical college and Hospital, Dharpur, Patan, Gujarat, India.
Skeletal TB (STB) contributes to around 10% of EPTB, and spinal TB has been the most common site of Skeleton TB (STB), amounting to around half of skeletal EPTB. . We report a rare case of a young male patient with spinal TB at L5- S1 level, which is uncommon.
Keywords: TB spine, Lumbosacral Junction, L5-S1 level
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Diploma in Orthopaedics, DNB Ortho Resident, GMERS medical college and Hospital, Dharpur, Patan, Gujarat, India. Email:  |
Maulik Patel, Ruchir Parmar, Mayur Vala, Pulkit Modi, TB spine at the level of lumbosacral junction ( L5-S1 Level ): A Case report. Surgical Rev Int J Surg Trauma Orthoped. 2022;8(6):35-39. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/262 |
 |
 ©
©  Figure 1A, B: Digital X-ray showing Lumbar spine anteroposterior view(1A) and lat view(1B). X-ray showing involvement of L5 and S1 vertebrae with loss of vertebral height.
Figure 1A, B: Digital X-ray showing Lumbar spine anteroposterior view(1A) and lat view(1B). X-ray showing involvement of L5 and S1 vertebrae with loss of vertebral height.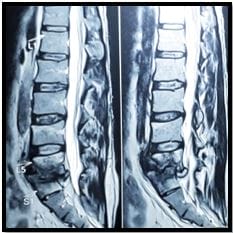 Figure: 2A
Figure: 2A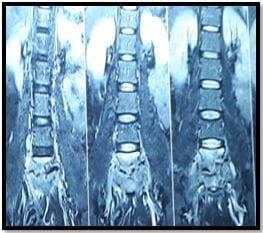 Figure: 2B
Figure: 2B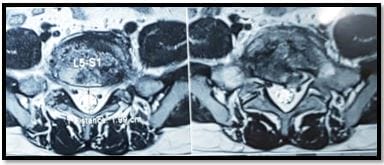 Figure: 2C
Figure: 2C Figure 3: x-ray lumbosacral spine: suggestive of fixation at L4-5, S1-2 with transforaminal lumbar interbody fusion.
Figure 3: x-ray lumbosacral spine: suggestive of fixation at L4-5, S1-2 with transforaminal lumbar interbody fusion.