Clinical study of miscellaneous causes of intestinal Obstruction
Chavan A.1, Keniya E.2*, Tamboli A.3, Degaonkar A.4, Kelkar V.5
DOI: https://doi.org/10.17511/ijoso.2021.i05.01
1 Aashish R Chavan, Assistant Professor, Department of General Surgery, Dr Shankarrao Chavan Government Medical College & Hospital, Nanded, Maharashtra, India.
2* Eshita B Keniya, Resident, Department of General Surgery, Dr Shankarrao Chavan Government Medical College & Hospital, Nanded, Maharashtra, India.
3 Abdul R Tamboli, Assistant Professor, Department of General Surgery, Dr Shankarrao Chavan Government Medical College & Hospital, Nanded, Maharashtra, India.
4 Anil Degaonkar, Associate Professor, Department of General Surgery, Dr Shankarrao Chavan Government Medical College & Hospital, Nanded, Maharashtra, India.
5 Vidyadhar Kelkar, Associate Professor, Department of General Surgery, Dr Shankarrao Chavan Government Medical College & Hospital, Nanded, Maharashtra, India.
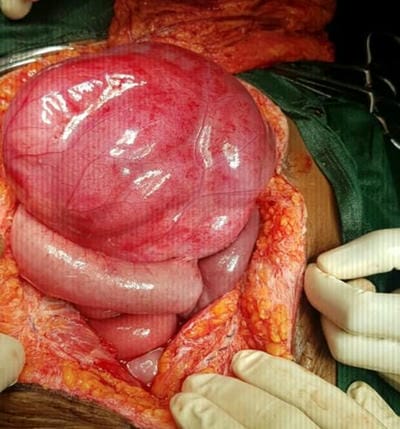
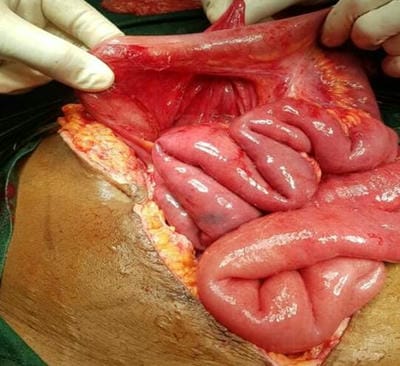
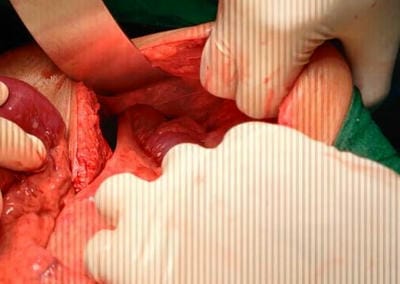
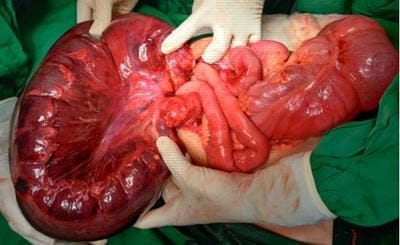
Aims and Objectives: Preoperative diagnosis of intestinal obstruction and timely intervention to reduce postoperative morbidity and mortality. Methods: A retrospective study of 124 cases of intestinal Obstruction from June 2018 to November 2020 by examining previous clinical records in terms of Clinical presentations, Laboratory investigations, Radiological investigations, Operative procedures, and Postoperative outcomes was done. Out of 124 cases, 40 cases were managed conservatively and were excluded from the study. Results: Out of 124 cases, 40 were managed conservatively, 30 with Adhesive Obstruction,20 with malignant growth, 14 with Obstructed External hernias and 20 with miscellaneous causes. There were 20 cases of rare causes of intestinal Obstruction, namely 2 Para duodenal hernia, two foreign body(phytobezoars) obstruction of ileum, 1 - Obstruction by worm infestation, 6 cases of volvulus, one gall stone ileus, 1meconium plug syndrome, and, 1 case of obstructed obturator hernia,1 case of Meckel's Diverticulum with Ileocolic Intussusception, five patients with the varied presentation of abdominal Koch's Out of 20 unusual causes, 17 cases were correctly diagnosed preoperatively by radiological investigations. 4 cases were managed with Resection and Anastomosis, five unusual cases presented with gangrenous changes and 2 cases needed ileostomy. Conclusion: These rare cases can be diagnosed early by a thorough history and clinical evaluation, and appropriate Radiological investigations to prevent hazardous gangrenous changes and prevent morbidity and mortality in patients.
Keywords: Intestinal Obstruction, Mortality, Morbidity, Radiological, Miscellaneous
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Resident, Department of General Surgery, Dr Shankarrao Chavan Government Medical College & Hospital, Nanded, Maharashtra, India. Email:  |
Aashish R Chavan et al: Clinical study of miscellaneous causes of intestinal Obstruction. Surgical Rev Int J Surg Trauma Orthoped. 2021;7(5):91-99. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/247 |
 |
 ©
©