Idiopathic Granulomatous Mastitis – Still an Enigma
Thomas V.1, George R.2, Nair L.3, Jojo J.4*
DOI: https://doi.org/10.17511/ijoso.2021.i05.05
1 Vijy Paul Thomas, MS, MRCSED, Professor, Department of General Surgery, MOSC Medical College and Hospital, Kolenchery, Ernakulam, Kerala, India.
2 Rahul George, MS, Assistant Professor, Department of General Surgery, MOSC Medical College and Hospital, Kolenchery, Ernakulam, Kerala, India.
3 Lakshmi Malavika Nair, MBBS, Junior Resident, Department of General Surgery, MOSC Medical College and Hospital, Kolenchery, Ernakulam, Kerala, India.
4* Joicy Els Jojo, MBBS, Junior Resident, Department of General Surgery, MOSC Medical College and Hospital, Kolenchery, Ernakulam, Kerala, India.
Introduction: Idiopathic granulomatous mastitis (IGM) is a chronic inflammatory disease of the breast, the aetiology of which has, as yet, not been fully established. The disease granulomatous mastitis was first described in the year 1972. Purpose: To date, there have been numerous reports regarding the symptoms, clinical examination, imaging findings and treatment options; however no protocol for evaluation and treatment has been established. Methods: A systematic search of the literature was performed using a defined search strategy and articles selected after adequate independent screening for suitability. The general understanding of the pathophysiology of the disease as well as the various methods of investigation and treatment employed in the various studies were analysed. Results: The most common modalities used for evaluation were ultrasound scans and mammograms with some role for MRI scans too. Core biopsy is ideal to obtain a tissue diagnosis. Regarding the treatment, many options have been successfully used of which antibiotics, steroids and surgery have been the most common. Conclusion: Consensus for an investigation and treatment protocol will require more studies in future.
Keywords: Mastitis, Granulomatous, Idiopathic
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , MBBS, Junior Resident, Department of General Surgery, MOSC Medical College and Hospital, Kolenchery, Ernakulam, Kerala, India. Email:  |
Vijy Paul Thomas, Rahul George, Lakshmi Malavika Nair, Joicy Els Jojo, Idiopathic Granulomatous Mastitis – Still an Enigma. Surgical Rev Int J Surg Trauma Orthoped. 2021;7(5):123-129. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/219 |
 |
 ©
© 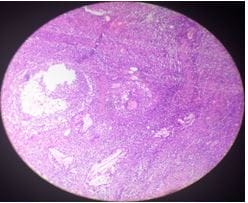 Figure 1:Low power view - granuloma H & E X40.
Figure 1:Low power view - granuloma H & E X40.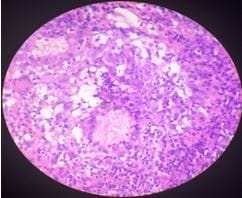 Figure 2: High power view - granuloma with cholesterol cleft and foreign body giant cell reaction H & E X100.
Figure 2: High power view - granuloma with cholesterol cleft and foreign body giant cell reaction H & E X100.