A rare case of superior ileocecal recess hernia
M. Illangovan1, Kumar K.2, Misra S.3*
DOI: https://doi.org/10.17511/ijoso.2020.i04.11
1 Illangovan M., Professor, Department of Surgery, Government Theni Medical College, Theni, Tamil Nadu, India.
2 K. Ashok Kumar, Assistant Professor, Department of Surgery, Government Theni Medical College, Theni, Tamil Nadu, India.
3* Shivanshu Misra, Consultant Gastro And Laparoscopic Surgeon, Shivani hospital and IVF Center, Kanpur, Uttar Pradesh, India.
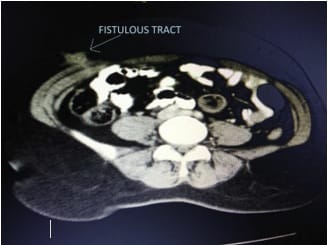
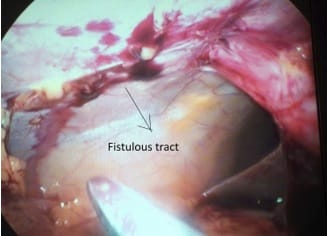
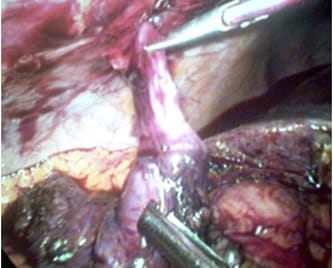
Internal hernias are a rare cause of small bowel obstruction, and one such internal hernia is superior ileocecal recess hernia, the subtype of pericycle hernia. The present study reports a case of small bowel obstruction due to superior ileocecal hernia for which laparotomy was performed. The surgery achieved a good outcome.
Keywords: Small bowel obstruction, Superior ileocecal recess hernia, small bowel obstruction, Internal hernia
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Consultant Gastro And Laparoscopic Surgeon, Shivani hospital and IVF Center, Kanpur, Uttar Pradesh, India. Email:  |
Illangovan M, Kumar KA, Misra S. A rare case of superior ileocecal recess hernia. Surgical Rev Int J Surg Trauma Orthoped. 2020;6(4):286-289. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/198 |
 |
 ©
©