Non-invasive preoperative assessment of ureteral stone impaction using peri-calculus ureteral thickness on Non-Contrast CT (NCCT) scan: A prospective Study
K Sharma P.1*, Aggarwal V.2, Baweja S.3, Nagori R.4, Katti P.5, Chhabra M.6
DOI: https://doi.org/10.17511/ijoso.2020.i02.01
1* Pradeep K Sharma, Associate Professor, Department of Urology, Dr. SN Medical College, Jodhpur, Rajasthan, India.
2 Vikas Aggarwal, Resident, Department of Urology, Dr. SN Medical College, Jodhpur, Rajasthan, India.
3 Shekhar Baweja, Resident, Department of Urology, Dr. SN Medical College, Jodhpur, Rajasthan, India.
4 Rupesh Nagori, Resident, Department of Urology, Dr. SN Medical College, Jodhpur, Rajasthan, India.
5 Pawan Katti, Resident, Department of Urology, Dr. SN Medical College, Jodhpur, Rajasthan, India.
6 M K Chhabra, Professor, Department of Urology, Dr. SN Medical College, Jodhpur, Rajasthan, India.
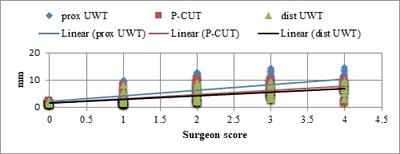
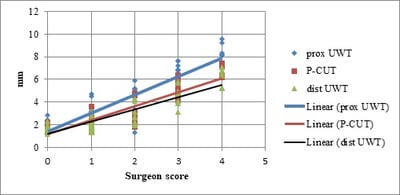
Background: Ureteral stone can be measured on the NCCT scan as peri-calculus ureteral thickness. If this depicts significant calculus impaction, the patient could be counseled regarding intra-operative risk and incomplete stone clearance. The present study was planned to evaluate the use of NCCT in patients with ureterolithiasis for the prediction of a favorable clinical outcome. Materials and methods: Patients who underwent ureterorenoscopy for ureteric calculus with pre-operative NCCT scan were included and intraoperative data were recorded. Operating surgeons were blinded for proximal ureteric wall thickness (p-UWT), peri-calculus ureteric wall thickness (p-CUT), and distal ureteric wall thickness (d-UWT) values. The guidewire was negotiated before each URS. Stone was considered impacted if guidewire could not be negotiated in 2 attempts. Results: Of total patients 108 patients, 70 patients had non-impacted calculus and 38 patients had impacted calculus. Patients with an impacted calculus had significantly higher p-UWT (9.76 ±3.11mm), p-CUT (6.82±2.57mm), and d-UWT (6.26±2.28mm) as compared to non-impacted. There was a positive correlation in SIS with p-UWT, p-CUT, and p-DWT in both impacted and non-impacted groups. Conclusion: Pre-operative ureteric wall thickness in proximal, peri, and distal to calculus can predict intraoperative risk and impaction of calculus.
Keywords: Ureteric thickness, Ureteral stone, NCCT, Stone impaction
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Urology, Dr. SN Medical College, Jodhpur, Rajasthan, India. Email:  |
Sharma PK, Aggarwal V, Baweja S, Nagori R, Katti P, Chhabra MK. Non-invasive preoperative assessment of ureteral stone impaction using peri-calculus ureteral thickness on Non-Contrast CT (NCCT) scan: A prospective Study. Surgical Review Int J Surg Trauma Orthoped. 2020;6(1):67-71. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/163 |
 |
 ©
©