Pneumothorax in Patients with Moderate to Severe Covid-19 Infection: A Retrospective Observational Study
George R.1, Paul Thomas V.2, Miriam Ipe S.3, Els Jojo J.4*
DOI: https://doi.org/10.17511/ijoso.2022.i01.03
1 Rahul George, Assistant Professor, Department of General Surgery, M.O.S.C Medical College & Hospital, Kolenchery, Ernakulam, Kerala, India.
2 Vijy Paul Thomas, Unit Chief and H.O.D, Department of General Surgery, M.O. S.C Medical College & Hospital, Kolenchery, Ernakulam, Kerala, India.
3 Shalini Miriam Ipe, Associate Professor, Department of Anesthesiology, M.O.S.C Medical College & Hospital, Kolenchery, Ernakulam, Kerala, India.
4* Joicy Els Jojo, Junior Resident, Department of General Surgery, M.O.S.C Medical College & Hospital, Kolenchery, Ernakulam, Kerala, India.
Background: Spontaneous pneumothorax as a complication of COVID-19 pneumonia is either uncommon or under-reported. The exact incidence and risk factors are still unknown. The objective of this study is to highlight an important complication, its incidence and explore the predisposing risk factors. Methods: We performed a retrospective review of COVID-19 pneumonia cases admitted to our hospital between February 2021 and June 2021. Data on their demographics, pre-existing risk factors, laboratory workup, imaging, treatment and clinical outcomes were gathered. Results: One thousand eight hundred and twenty-five patients have admitted to our institution between February 2021 and June 2021 with COVID-19 infection. 11 patients developed a pneumothorax (0.6%). 6 out of the 11 cases were patients who required mechanical ventilation (54.5%). All of these patients underwent chest tube insertion. Baseline imaging of these patients showed ground-glass opacities (GGO) and consolidation. 8 of the 11 patients succumbed to the disease (72.7%). Conclusion: In patients admitted with COVID-19 pneumonia and developing sudden respiratory compromise, pneumothorax is an important complication to be considered. Prompt identification of this complication and timely intervention is necessary to reduce morbidity and mortality. Low tidal volume lung-protective ventilation and the use of non-invasive ventilation for oxygenation remain the cornerstone in the management of COVID pneumonia. It significantly decreases iatrogenic complications like VILI (ventilator-induced lung injury) and P-SILI (patient self-inflicted lung injury.
Keywords: COVID-19, Pneumomediastinum, Pneumonia, Pneumothorax, Ventilation
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Junior Resident, Department of General Surgery, M.O.S.C Medical College & Hospital, Kolenchery, Ernakulam, Kerala, India. Email:  |
Rahul George, Vijy Paul Thomas, Shalini Miriam Ipe, Joicy Els Jojo, Pneumothorax in Patients with Moderate to Severe Covid-19 Infection: A Retrospective Observational Study. Surgical Rev Int J Surg Trauma Orthoped. 2022;8(1):12-23. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/256 |
 |
 ©
© 

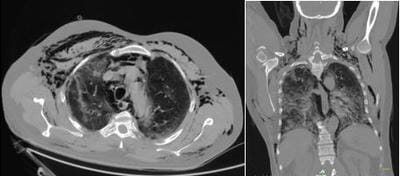 Figure 2: Axial and Coronal Sections of Ct Imaging Showing Ground Glass Opacities, Subcutaneous Emphysema, Pneumomediastinum and Pneumothorax.
Figure 2: Axial and Coronal Sections of Ct Imaging Showing Ground Glass Opacities, Subcutaneous Emphysema, Pneumomediastinum and Pneumothorax.