A Case Report on Primary Large Bowel Lymphoma
Shree Venkatesan B.1*, Senthil Kumar k.2, Thangamani P.3
DOI: https://doi.org/10.17511/ijoso.2022.i01.04
1* Bhaskaran Shree Venkatesan, Postgraduate, , MMC, Chennai, Tamil Nadu, India.
2 k Senthil Kumar, Assistant Professor, , MMC, Chennai, Tamil Nadu, India.
3 P Thangamani, Professor, Chief of General Surgery, MMC, Chennai, Tamil Nadu, India.
Large bowel (colorectal) lymphoma is a very rare tumor, accounting for <0.5% of primary colorectal malignancies, ~1.5% of all lymphomas, and ~15% of gastrointestinal lymphoma. The definition of primary GI lymphoma has differed among authors but typically refers to lymphoma that predominantly involves any section of the GI tract from the oropharynx to the rectum. The major site of extranodal non-Hodgkin lymphoma is the gastrointestinal tract(stomach>small intestine >large intestine). The disease appears later in life, predominantly in the male population. Complaints are nonspecific, requiring a high index of suspicion to establish the diagnosis Treatment includes surgery/chemotherapy/radiotherapy or a combination of all these three modalities. The aim of this paper is to report a rare case of primary colon lymphoma in a female patient.
Keywords: Large bowel lymphoma, Colorectal lymphoma, Primary
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Postgraduate, , MMC, Chennai, Tamil Nadu, India. Email:  |
Bhaskaran Shree Venkatesan, k Senthil Kumar, P Thangamani, A Case Report on Primary Large Bowel Lymphoma. Surgical Rev Int J Surg Trauma Orthoped. 2022;8(1):24-28. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/252 |
 |
 ©
©  Fig 1: Right hemicolectomy specimen Final biopsy report.
Fig 1: Right hemicolectomy specimen Final biopsy report.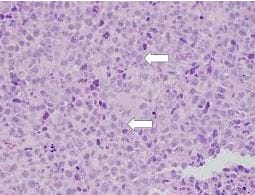 Fig 2: sheets of lymphocyte aggregates.
Fig 2: sheets of lymphocyte aggregates.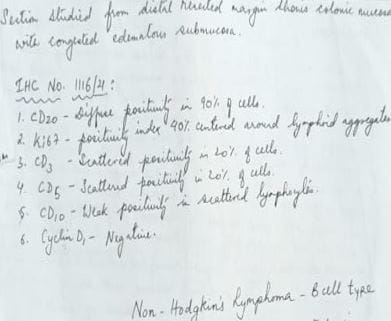 Fig 3: Final biopsy report.
Fig 3: Final biopsy report.