A Clinical Study to Compare Functional Outcome of Proximal Humerus Fracture in Adults (18- 80yrs) Treated By Philos Platting and Conservative Modalities
Jetpariya D.1, Patel B.2*, Patel P.3, Patel H.4
DOI: https://doi.org/10.17511/ijoso.2021.i05.03
1 Divyesh Pragajibhai Jetpariya, Senior Resident, Department Of Orthopedics, M.P Shah Medical College, Jamnagar, Gujarat, India.
2* Baiju Mukeshbhai Patel, Senior Resident, Department Of Orthopedics, Smt. NHL Municipal Medical College, Ahmedabad, Gujarat, India.
3 Parth Pravinbhai Patel, Final Year MBBS, Department Of Orthopedics, C U Shah Medical College, Surendranagar, Gujarat, India.
4 Harsh Girishbhai Patel, Senior Resident, Department Of Orthopedics, Banas Medical College, Palanpur, Gujarat, India.
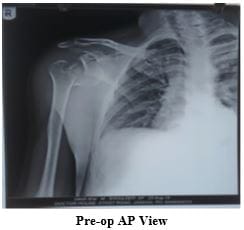
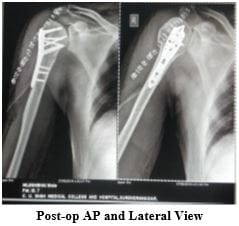
Introduction: It is the commonest fracture affecting the shoulder girdle in adults. Proximal humeral fractures account for almost 7% of all fractures and make up 80% of all humeral fractures. The purpose of this study is to carry out to enlighten functional outcome fracture proximal humerus treated with conservative and PHILOS platting and comparison of that. Material and Method: Twenty-six patients attended the Department Of Orthopaedics from May 2018 to August 2020 and were involved in this study prospectively, out of which 11 were male, and 15 were female. They were analysed clinically and radiologically using Constant and Murley shoulder scoring criteria. Out of 26 cases, 12 were treated conservatively, and 14 were treated by Pen reduction internal fixation (ORIF) Result: Out of 12 patients treated conservatively, three had excellent, seven had good, and 2 had fair functional outcome, whereas 14 patients treated by open reduction and internal fixation two had excellent, 4 had good, four had fair, and 4 had the poor functional outcome. Complications were seen in 9 patients. Out of that, five patients had shoulder stiffness, 3 had malunion, and 1 had impingement of implant. Conclusion: Proximal humerus fracture occurred most commonly in the 4th to 6th decade of life. For minimally displaced fracture, treatment of choice is nonoperative. For 2 part fracture treated with conservative modalities showed slightly better results than operated patients, but for 3 part fracture operated patients had somewhat better results than conservative.
Keywords: Proximal Humerus, Philos Plate, Shoulder Stiffness
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior Resident, Department Of Orthopedics, Smt. NHL Municipal Medical College, Ahmedabad, Gujarat, India. Email:  |
Divyesh Pragajibhai Jetpariya, Baiju Mukeshbhai Patel, Parth Pravinbhai Patel, Harsh Girishbhai Patel, A Clinical Study to Compare Functional Outcome of Proximal Humerus Fracture in Adults (18- 80yrs) Treated By Philos Platting and Conservative Modalities. Surgical Rev Int J Surg Trauma Orthoped. 2021;7(5):108-115. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/245 |
 |
 ©
©