Clinicopathological study of carcinoma gallbladder and its management: a prospective study in a tertiary care hospital in Central India
Koshariya M.1, Suroshe T.2*, Alex S.3, Rajput G.4, K M G.5, Vaidya K.6, Shukla S.7, Patel B.8, Shalini M.9, MC S.10
DOI: https://doi.org/10.17511/ijoso.2020.i04.01
1Mahim Koshariya, Professor, 2*Tushar Suroshe, Resident, 3Sharon Alex, Resident, 4Gaurav Rajput, Resident, 5Guka Priyan K M, Resident, 6Kunal Vaidya, Resident, 7Shikha Shukla, Resident, 8Badri Patel, Resident, 9Megha Shalini, Resident, 10Songra MC, Professor and Head; all authors are affiliated with the Department of Surgery, Gandhi Medical College and Associated Hamidia Hospital, Bhopal, Madhya Pradesh, India.
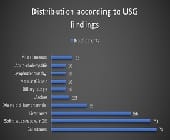
Background: Gallbladder cancer is a highly aggressive malignancy of the biliary system having the shortest median survival rate. Being aggressive biological nature and lack of sensitive screening test for early detection it has a poor prognosis. Aim: The purpose is to study the relative frequency of gallbladder cancer in reference to age, sex, etiological factors, clinical signs and symptoms in relation to the stages and the outcomes of different treatment modalities. Methods: This study is observational and conducted in the Department of General Surgery Gandhi Medical College and Aassociated Hamidia Hospital, Bhopal, Madhya Pradesh, during the period of 2017-2019. all patients who came themselves to OPD were evaluated further. Results: This study shows that majority of the patients were elderly females. Most of them presented with pain in the right hypochondrium found in 78 patients (78%), nausea and vomiting in 36 patients (36%), and jaundice in 30 patients (30%). Tenderness in the right hypochondrium (85%), anemia (78%) followed by weight loss (68%) were the three commonest signs. Conclusion: Gallbladder cancer is an aggressive malignancy of the biliary tract and has high case fatality with shortest median survival rates.
Keywords: Gallbladder cancer, Gallstones, Aggressive malignancy
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Resident, Department of Surgery, Gandhi Medical College and Associated Hamidia Hospital, Bhopal, Madhya Pradesh, India. Email:  |
Koshariya M, Suroshe T, Alex S, Rajput G, Guka Priyan K M, Vaidya K, Shukla S, Patel B, Shalini M, Songra MC. Clinicopathological study of carcinoma gallbladder and its management: a prospective study in a tertiary care hospital in Central India. Surgical Rev Int J Surg Trauma Orthoped. 2020;6(4):223-231. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/197 |
 |
 ©
©