Evaluation of the significance of Alvarado score in the diagnosis of acute appendicitis in tribal area
K. Kulkarni R.1*
DOI: https://doi.org/10.17511/ijoso.2020.i02.10
1* Ravindra K. Kulkarni, Associate Professor, Department of Surgery, Zydus Medical College and Hospital, Dahod, Gujarat, India.
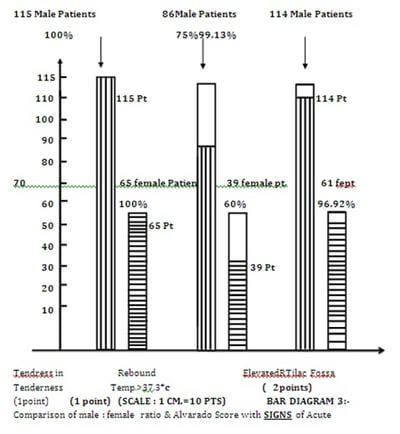
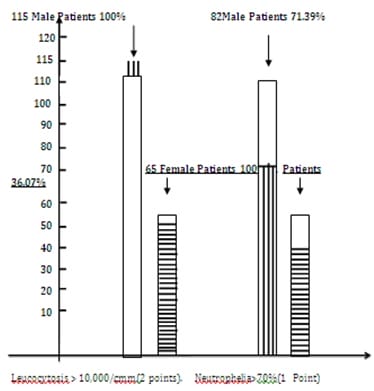
Background: Acute Appendicitis is a common surgical emergency which even with modern diagnostic facilities remains a challenging task for the surgeon. The variation in the presentation can confuse even experienced surgeons. On looking at the literature, it was found that a negative Appendicectomy rate has been consistently mentioned Aim: The following study was therefore conducted for Evaluation Of Significance Of Alvarado Score In Diagnosis Of Acute Appendicitis In Tribal Area. This is an old standard scoring system, very economical, noninvasive, and revalidation was done in the tribal area to reach the diagnosis. Material and Methods: A Study of 180 patients of acute appendicitis was conducted in tribal areas and Alvarado score carries high significant value in diagnosis and management of acute appendicitis. The period to study was from August 2018 to January 2020. Result: 180 patients were subjected to Appendicectomy. Out of the 33 were operated by laparoscopy (18.33%). All the Appendicectomy specimens were studies macroscopically and microscopically. All the specimens were cut open and inspected for pathology. Conclusion: The present study concludes that the Alvarado score, an economical, noninvasive clinical scoring system, carries high significant value in the diagnosis and management of acute appendicitis in the tribal area.
Keywords: Alvarado Score, Acute Appendicitis, Appendicectomy, Tenderness, Rebound tenderness
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Surgery, Zydus Medical College and Hospital, Dahod, Gujarat, India. Email:  |
Ravindra KK. Evaluation of the significance of Alvarado score in the diagnosis of acute appendicitis in tribal area. Surgical Review Int J Surg Trauma Orthoped. 2020;6(2):127-133. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/175 |
 |
 ©
©