Study of surgical management of trochanteric fracture of the femur with dynamic hip screw
D Rao R.1, PV Chowdary R.2*, Aditya K.3, Deedi K.4
DOI: https://doi.org/10.17511/ijoso.2020.i02.04
1 Rama D Rao, Associate Professor, Department of Orthopedics, GSL Medical College, Rajamahendravaram, Andhra Pradesh, India.
2* Ramana PV Chowdary, Assistant Professor, Department of Orthopedics, GSL Medical College, Rajamahendravaram, Andhra Pradesh, India.
3 Aditya K, Resident, Department of Orthopedics, GSL Medical College, Rajamahendravaram, Andhra Pradesh, India.
4 Kiran Deedi, Central Research Laboratory, GSL Medical College, Rajamahendravaram, Andhra Pradesh, India.
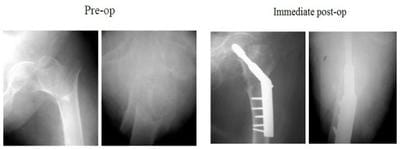
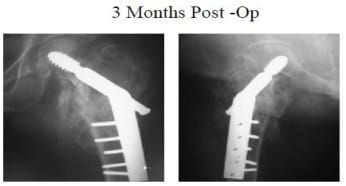
Background: The use of a dynamic hip screw (DHS) for stable trochanteric hip fracture fixation has been successfully applied in fracture healing for more than 20years. DHS fixation on unstable trochanteric fractures still has a more failure rate, particularly in osteoporosis patients. Thus, this study is aimed to investigate the biomechanical property of the DHS system to provide the lesser trochanter fragment stable fixation. Material and methods: This cross-sectional, observational, and follow-up study was conducted in the Department of Orthopedics, GSL Medical College and General Hospital, Rajamahendravaram with a total of 40 cases of trochanteric fractures. All surgeries were performed under spinal anesthesia. Surgery done was an internal fixation with DHS and 135-degree angled blade plate. Results: Among 40 cases, 32.5% were Type I, and 67.5% were Type II Trochanteric fractures. 40% cases had grade 3 osteoporosis and 30% had grade4-osteoporosis rest of the patients were having grade 2 (20%), grade 5 (7.5%), grade 6 (2.5%) and grade1 (0%), according to Singh’s index. The clinical and functional outcomes of the procedure were excellent in 10 hips (25%), Good in 20 hips (50%), Fair in 6 hips (15%), and 4 (10%) of the patients had poor results. Conclusions: Trochanteric fractures are essentially fractured of the elderly, with osteoporotic bones. The dynamic hip screw is the operative treatment of choice for stable trochanteric fractures.
Keywords: Fracture, Hip, Trochanteric, and dynamic hip screw
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Orthopedics, GSL Medical College, Rajamahendravaram, Andhra Pradesh, India. Email:  |
Rao RD, Chowdary RPV, Aditya K, Deedi K. Study of surgical management of trochanteric fracture of the femur with dynamic hip screw. Surgical Review Int J Surg Trauma Orthoped. 2020;6(2):87-92. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/169 |
 |
 ©
©