A study of functional outcome of bimalleolar fracture treated with fully threaded 4 mm cancellous cannulated screw in medial malleolus fracture
P Vala G.1, Patel N.2*, Vora J.3
DOI: https://doi.org/10.17511/ijoso.2020.i02.02
1 Gaurav P Vala, Assistant Professor, CU Shah Medical College and Hospital, Surendranagar, Gujarat, India.
2* Neel Patel, Resident, CU Shah Medical College and Hospital, Surendranagar, Gujarat, India. https://orcid.org/0000-0002-2570-7155
3 Jinesh Vora, Associate Professor, CU Shah Medical College and Hospital, Surendranagar, Gujarat, India.
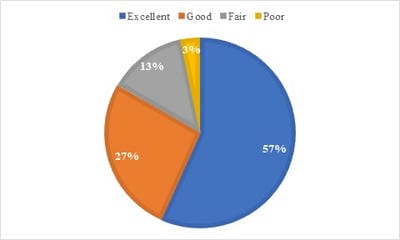
Aim: To analyse the functional outcome of Medial malleoli after Internal Fixation of medial malleolar fracture with fully threaded 4 mm cancellous cannulated screws. Introduction: Ankle fractures are one of the commonest fractures encountered by an orthopaedic surgeon with the majority being treated with open reduction and tension band wiring but it has a midterm and long term complications like hardware prominence, low-grade infection and hardware removal. Purpose of this study on medial malleolus fracture is to evaluate functional outcome after open reduction and fully threaded 4 mm cancellous cannulated screw fixation which has a very low complication rate. Materials and Method: This is a prospective study done in c u shah medical college and hospital Surendranagar. In the present study 30 cases of bimalleolar ankle fracture.Common Mechanism of Injury was Road traffic accidents and fall from height. the diagnosis was confirmed by Anteroposterior, lateral and Mortise radiograph. Classifications used are Lauge-Hanse Classification and DenisWeber Classification. Fully threaded 4 mm Cannulated cancellous screw was used for medial malleolus fixation. Post-op protocol: Postoperatively limb were immobilized in a plaster splint for 6 weeks and limb were elevated. Results: According to Baird and Jackson scoring system out of 30 cases, 56.67% were excellent and 26.67% were good, 13.34% were fair and 3.32% were poor. Conclusion: Open reduction and tension band wiring fixation of medial malleolus has biomechanically proved stable fixation but it has a midterm and long term complications like hardware prominence, low-grade infection and hardware removal.
Keywords: Medial malleolus, 4mm fully threaded cancellous cannulated screw
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Resident, CU Shah Medical College and Hospital, Surendranagar, Gujarat, India. Email:  |
Vala GP, Patel N, Vora J. A study of functional outcome of bimalleolar fracture treated with fully threaded 4 mm cancellous cannulated screw in medial malleolus fracture. Surgical Review Int J Surg Trauma Orthoped. 2020;6(2):72-78. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/159 |
 |
 ©
©