Evaluation of modified Alvarado scoring system and RIPASA scoring system as diagnostic tools of acute appendicitis
Kumar A.1*, Snehlata2
DOI: https://doi.org/10.17511/ijoso.2020.i01.03
1* Abhishek Kumar, Specialist Doctor, Department of General Surgery, Sadar Hospital Hazaribag and Visiting Consultant at Vandana Nursing Home and IVF Clinic, Hazaribag, Jharkhand, India.
2 Snehlata, Specialist Doctor, Department of obst. and gynaec, Sadar Hospital Hazaribag and Visiting Consultant at Vandana Nursing Home and IVF Clinic, Hazaribag, Jharkhand, India.
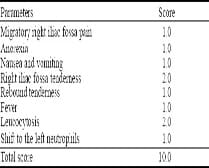
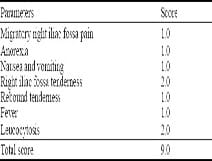
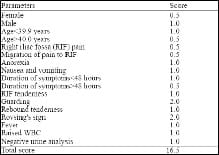
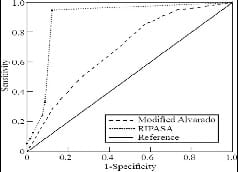
Background: Acute appendicitis is the most common surgical condition presented in emergency departments worldwide. Clinical scoring systems, such as the Alvarado and modified Alvarado scoring systems, were developed with the goal of reducing the negative appendectomy rate to 5%–10%. The Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) scoring system was established in 2008 specifically for Asian populations. The aim of this study was to compare the modified Alvarado with the RIPASA scoring system in Kuwait population. Methods: This study included 90 patients who underwent appendectomies and were documented as having "acute appendicitis" or "abdominal pain" in the operating theatre register from June 2014 to May 2018. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), diagnostic accuracy, predicted negative appendectomy and receiver operating characteristic (ROC) curve of the modified Alvarado and RIPASA scoring systems were derived using SPSS statistical software. Results: A total of 68 patients were included in this study according to our criteria. The cut-off threshold point of the modified Alvarado score was set at 7.0, which yielded a sensitivity of 82.8% and a specificity of 56%. The PPV was 89.3% and the NPV was 42.4%. The cut-off threshold point of the RIPASA score was set at 7.5, which yielded a 94.5% sensitivity and an 88% specificity. The PPV was 97.2% and the NPV was 78.5%. The predicted negative appendectomy rates were 10.7% and 2.2% for the modified Alvarado and RIPASA scoring systems, respectively. Conclusion: Based on the results of this study, the RIPASA score is a simple scoring system with better sensitivity and specificity than the modified Alvarado scoring system in Asian populations. It consists of 14 clinical parameters that can be obtained from a good patient history, clinical examination and laboratory investigations.
Keywords: Acute appendicitis, Modified Alvarado score, RIPASA score
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Specialist Doctor, Department of General Surgery, Sadar Hospital Hazaribag and Visiting Consultant at Vandana Nursing Home and IVF Clinic, Hazaribag, Jharkhand, India. Email:  |
Kumar A, Snehlata, Evaluation of modified Alvarado scoring system and RIPASA scoring system as diagnostic tools of acute appendicitis. Surgical Review Int J Surg Trauma Orthoped. 2020;6(1):15-20. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/145 |
 |
 ©
©