Role of laparostomy in preventing early morbidity and mortality in advanced peritonitis patients
Gurram L.1, Inamdar P.2*, Manogyna D.3
DOI: https://doi.org/10.17511/ijoso.2020.i01.01
1 Laxmikanth Gurram, Assistant Professor, Department of Surgery, Mamata Medical College and hospital, Khammam, Telangana, India.
2* Padmanabh Inamdar, Associate Professor, Department of Surgery, Mamata Medical College and hospital, Khammam, Telangana, India.
3 Manogyna D., Junior Resident, Department of Surgery, Mamata Medical College and hospital, Khammam, Telangana, India.
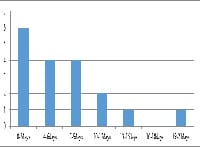
Background: Very few studies are available for the indication and the need of laparostomy in cases of faecal, biliary peritonitis and gangrenous bowel. The open abdomen procedure is one of the greatest surgical advances in recent times, avoiding the development of abdominal compartment syndrome. Methods: The present study was a prospective study of the patients who underwent laparostomy during 2yrs study period. Patients who met the inclusion criteria were included in the study. The indications, complications and outcomes of the study were noted. Results: Majority of the patients are in the age group of 31 to 40yrs. With laparostomy and damage control surgery recovery was seen in 86.6% patients. Post-operative complications were seen in 33.3% of the patients, with electrolyte imbalance, enterocutaneous fistula, anastomotic leak being the most common complications. Deaths were secondary to septicaemia with mortality rate 16.6%. Conclusion: Laparostomy or open abdomen is a useful emergency measure in certain conditions where there is a need for re-exploration for abdomen and cannot be closed due to gross edema and contamination. It reduces operative time and also facilitates re-look operations.
Keywords: Laparostomy, Open abdomen, Septicemia, Relook surgery
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Surgery, Mamata Medical College and hospital, Khammam, Telangana, India. Email:  |
Gurram L, Inamdar P, Manogyna D. Role of laparostomy in preventing early morbidity and mortality in advanced peritonitis patients. Surgical Review Int J Surg Trauma Orthoped. 2020;6(1):1-7. Available From https://surgical.medresearch.in/index.php/ijoso/article/view/142 |
 |
 ©
©